
The gastric bypass is a short circuit made in the stomach. The operation reduces the size of the stomach in order to limit the quantities of food ingested.
Gastric bypass is an obesity surgery technique aimed at adults suffering fromsevere obesity (BMI greater than 40 kg/m² or BMI between 35 and 40 associated at least one complication that surgery can improve).
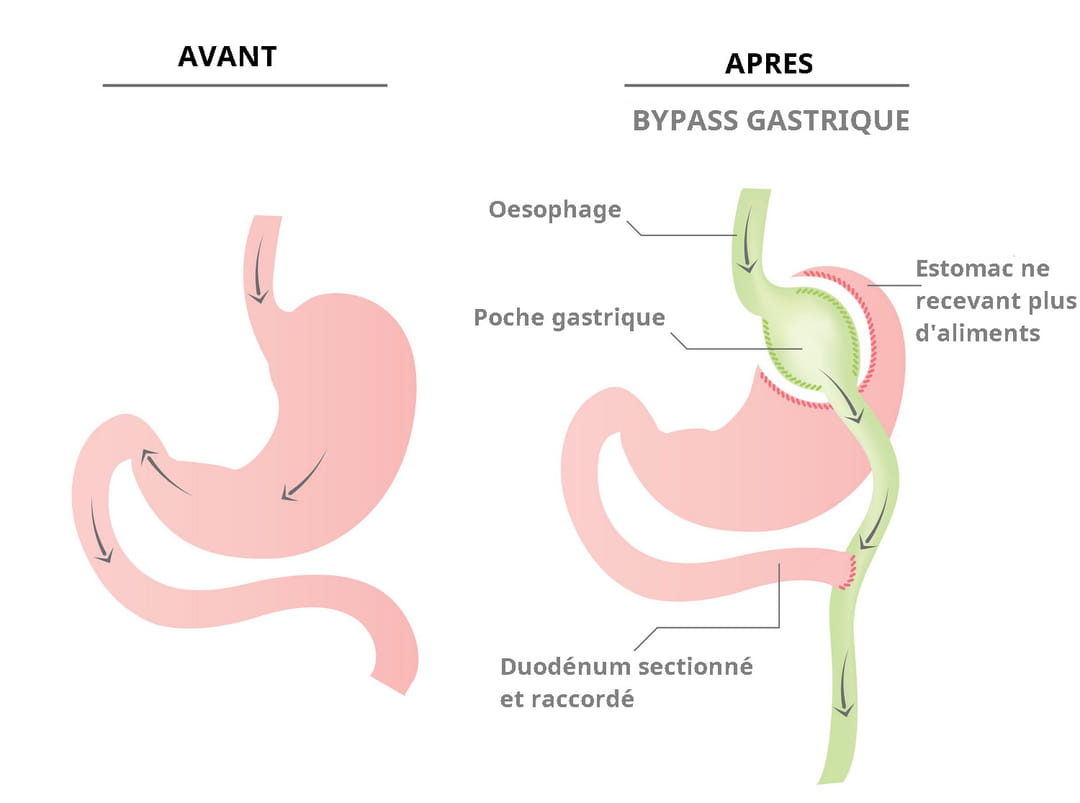
Gastric bypass is a surgical technique which consists of bypass a large part of the stomach and reduce it to a small stomach pouch, to reduce the quantity of foods ingested and their assimilation by the body. Food goes directly to the middle part of the small intestine. The Bypass is a definitive anatomical modification although it may be reversible in certain cases.
There are two bypass techniques: Roux-en-Y bypass (BPGY) (oldest, most evaluated and most frequently practiced method) and the gastrojejunal bypass said in “omega” (BPGO). The BPGY has been reimbursed by Health Insurance since March 2005 and validated by the High Authority of Health (HAS). However, for the BPGO, the latter is more suspicious. In a communicated published in September 2019, she emphasizes that her practice “has spread in recent years, in France, without prior assessment, and without specific monitoring being possible. His appeal is debated among bariatric surgeons. After evaluation, HAS estimated that the BPGO made with a 200 cm handle “notit did not constitute a validated technique (and) is therefore not an alternative to Roux-en-Y gastric bypass.” The one made with a 150 cm handle is too poorly documented, according to the HAS, to be considered effective and safe. HAS concluded that this technique of Omega bypass does not represent a relevant alternative to the Y bypass and recommends that it not be reimbursed by Health Insurance. “Indeed, studies reveal a greater number of serious complications – including severe deficiencies, particularly in vitamins and minerals, reflux biliary… In addition, there is no conclusive data on better effectiveness of the omega bypass compared to the Y bypass.”
The average expected excess weight loss isapproximately 65% at 5 yearswhich corresponds to approximately a decrease of approximately 35 to 40 kg. Weight loss is important from the first 3 months and causes significant fatigue. The patient not only loses fat but also muscle, hence the need to return to regular physical activity quickly. Bypass has been practiced for decades and has proven itself in terms of weight loss in people withclinically severe obesity.
| The choice of surgical technique is decided by a multidisciplinary team in agreement with the person concerned. Many criteria are taken into account, including: the experience and technical environment of the surgeon and the anesthesia team, the extent of obesity, BMI, age, medical history and surgical procedures, associated digestive pathologies, the presence of type 2 diabetes, current treatments and eating disorders. |
Creating a Bypass concerns the teenagers and the adults. The affected person must suffer from clinically severe obesity for which other treatments have not worked. Her BMI must be greater than 40 Or “be between 35 and 40 if it is associated with complications linked to obesity” specifies Dr Vincent Frering. A complication such as diabetes, high blood pressure, severe sleep apnea, hip or knee osteoarthritis, metabolic diseases. Furthermore, the patient must accept the idea of preparation and lifelong monitoring with a profound modification of his eating habits.
As highlighted by Dr Frering, bariatric surgeon in Lyon “Preparation is essential in obesity surgery. It gives better results. We cannot do obesity surgery if there is not good supervision around it”. For adults, the preoperative follow-up is at least 6 monthsit includes dietary consultations to set up a new diet which must be maintained, the resumption of physical activity, psychological help if the patient feels the need. “If the preparation is not optimal, we increase the risk of reflux and weight regain” warns the professional.
The duration of the intervention lasts between 1h30 and 3h and is done under general anesthesia, usually under laparoscopy. Hospitalization varies depending on individuals and establishments, it is between 2 and 8 days. Resumption of work for sedentary people can generally be done after 2 weeks.
Bypass complications are rare, but should be known. The risk of mortality is approximately 0.5%. “The most common complications are fistulas in 2 to 4% of operations, and hemorrhages in 1% of cases, explains Dr. Frering. To which are added risks ulcerof refluxmalnutrition and vitamin deficiencies” types B1, B12, B6, but also iron, calcium and zinc. Ulcer, narrowing at the junction between the stomach and intestine, a occlusion of the intestine are also among the complications that can occur, such as episodes of hypoglycemia or dumping syndrome (feeling of uneasiness accompanied by palpitations, headaches, nausea, etc.) after meals. Episodes of constipation may also appear.
Whatever the technique used, a bariatric operation subsequently imposes, and for life:
- to maintain your new eating habits and practice regular physical activity adapted to your case
- to be followed regularly by the multidisciplinary team which carried out the intervention, in liaison with your treating doctor (at least 4 consultations in the first year).
The power supply after making a Bypass is the same as for the other techniques, namely: “Eat liquid for a week, then introduce soft and mixed foods for 15 days and reintroduce the rest of the foods gradually, enlightens Dr. Frering. You just have to avoid carbonated drinks which dilate the pockets.”
Bypass is never performed during pregnancy. A pregnancy test must always be carried out before any possible operation. However, “The Bypass is compatible with pregnancy, assures Dr. Frering. It is rather obesity which is not really compatible. For many women, sterility can be due to obesity. And once they have lost weight, they become fertile again. In the case of a pregnancy after Bypass, supplementation with iron, folate, vitamin B12, vitamin D and calcium will be prescribed.
The cost of the operation is quite high, plus the various consultations with the medical team. Health insurance reimburses up to 70% surgical intervention and hospitalization if the request for prior agreement has been completed and accepted by the medical advisor. The intervention must be carried out in one of the 37 Specialized Obesity Centers to be covered by health insurance. Please note, certain health procedures and products are not reimbursed by Health Insurance. This is particularly the case for vitamin supplements and most protein supplements; consultations with a psychologist or dietitian outside the multidisciplinary team, certain biological procedures (vitamin B1 dosage), excess fees from doctors (according to the mutual insurance contract). To avoid disappointments, always seek the advice of the multidisciplinary team, the health insurance fund or the mutual insurance company.
Failures can occur, they are mainly linked to poor monitoring and poor compliance with post-operative recommendations such as the need to change eating behavior and resumption of regular physical activity.
Thanks to Dr Vincent Frering, bariatric surgeon in Lyon.